(Psychology)
Maladaptive eating behaviour features in a range of psychopathologies. A recent report on national attitudes towards mental health and addiction in New Zealand found widespread concern for the prevalence of eating disorders among young people, as well as limited access to specialist treatment for those with these disorders (Mental Health and Addiction Inquiry, 2018).
The concern is not misplaced, with a lifetime prevalence among New Zealanders for developing an eating disorder at 1.7% (Ministry of Health, 2008). Eating disorders can be characterised by either insufficient or excessive caloric intake, however the focus of this current project is on the latter. Specifically, binge eating behaviour is defined by excessive caloric intake within a short period of time, referred to as binge episodes. Binge eating features in two disorders, Binge-Eating Disorder (BED) and Bulimia Nervosa (BN). Binge episodes are the central feature of BED, which typically includes rapid consumption of food until the onset feelings of uncomfortable fullness, even when the individual may not have been physically hungry (American Psychiatric Association, 2013). BN, by contrast, includes the addition of purging behaviours to prevent weight gain, which is typically performed via self-induced vomiting, or the abuse of laxatives (American Psychiatric Association, 2013).
Binge eating behaviour has been the target of many interventions in recent decades, with some proving more efficacious than others. For instance, a systematic review of third-wave behavioural therapies found that Cognitive Behavioural Therapy (CBT) was associated with greater pre-post effect sizes than other interventions (Linardon, Fairburn, Fitzsimmons-Craft, Wilfley, & Brennan, 2017). In addition, CBT has proven to be more efficacious than behavioural interventions targeting weight loss, specifically when the version of CBT being delivered is tailored to the unique behaviours of binge eaters (Linardon, Wade, de la Piedad Garcia, & Brennan, 2017). For example, Appetite-Focused CBT (CBT-A) addresses symptoms pertaining to appetite such as inhibited recognition of, and response to internal signals of hunger and satiety (Virginia V. W. McIntosh, Jordan, Carter, Latner, & Wallace, 2007). Eating in response to internal signals is referred to as Intuitive Eating (IE) and is a common treatment goal in binge eating interventions.
The purpose of this conceptual review is to outline the role of internal signals in characterising both binge eating and IE by connecting parallel threads of research in the wider literature. Firstly, it will be briefly argued that the presence and nature of environmental risk factors for binge eating suggests that this behaviour is a conditioned response to external stimuli.
Proceeding from this is a theoretical outline detailing the process of classically conditioning stimuli, either physiologically or environmentally sourced, as appetite cues, as well as a description of how cues result in different eating patterns. This framework informs the remainder of the review and draws heavily on the classical conditioning model of binge eating outlined by Jansen (1998).
The third component of the review outlines deficits in the ability to recognise internal signals (referred to as ‘interoceptive awareness’) among those with binge eating problems and concludes that targeting this interoceptive deficit is critical to ensure long-term success in the treatment of these disorders.
The fourth aspect describes how IE interventions are a form of interoceptive conditioning, which conditions internal physiological signals as appetite cues to regulate food intake. The review then concludes with implications and limitations around both the underlying theory behind IE, as well as within the literature that supports it.
Proceeding from this is a theoretical outline detailing the process of classically conditioning stimuli, either physiologically or environmentally sourced, as appetite cues, as well as a description of how cues result in different eating patterns. This framework informs the remainder of the review and draws heavily on the classical conditioning model of binge eating outlined by Jansen (1998).
The third component of the review outlines deficits in the ability to recognise internal signals (referred to as ‘interoceptive awareness’) among those with binge eating problems and concludes that targeting this interoceptive deficit is critical to ensure long-term success in the treatment of these disorders.
The fourth aspect describes how IE interventions are a form of interoceptive conditioning, which conditions internal physiological signals as appetite cues to regulate food intake. The review then concludes with implications and limitations around both the underlying theory behind IE, as well as within the literature that supports it.
Environmental Risk Factors for Binge Eating
The literature on developmental psychopathology is saturated with accounts outlining the role of environmental risk factors in developing disordered eating behaviours. Childhood home environments, specifically those characterised by strict and abusive parenting, is a risk factor with much supporting literature. For example, national survey data from the United States found that child maltreatment, such as abuse and neglect, were associated with diagnoses of BN and BED among both men and women (Afifi et al., 2017). In addition, a systematic review of the relationship between parental bonding and eating disorders among women found that eating disorders were associated with lower self-reported levels of childhood parental affection and warmth (Tetley, Moghaddam, Dawson, & Rennoldson, 2014). Recently, researchers have specified which parental behaviours contribute to the onset of eating disorders. The invalidation of expressions of internal states by children, either by minimising or punishing these expressions, has been associated with a range of psychopathologies, including Borderline Personality Disorder, which exhibits much diagnostic overlap with both BN and BED (American Psychiatric Association, 2013; Linehan, 1993).
In addition, direct support for the relationship between childhood invalidation and the onset of eating disorders exists within the literature. In developing a scale to measure childhood invalidation among both clinical and non-clinical samples of individuals with disordered eating patterns, Mountford, Corstorphine, Tomlinson, and Waller (2007) found that individuals who scored higher on invalidation were more likely to score higher on measures of eating pathology, and speculated that this relationship may be mediated by emotional regulation skills. Further, a study by Haslam, Arcelus, Farrow, and Meyer (2012) measuring childhood invalidation, eating pathology, and attitudes towards emotional expression among a non-clinical sample of young women found similar results.
Specifically, they found that the relationship between invalidation and eating pathology was mediated by normative beliefs about the propriety of emotional expressions. In other words, a negative attitude towards emotional expression, which may be procured from an invalidating environment, presented a risk factor for disordered eating.
One implication of these findings is that childhood environments contribute to the way in which we understand and respond to our internal states, such as emotions or, by extension, other internal biochemical signals such as hunger.
Conditioning Appetite Cues
Specifically, they found that the relationship between invalidation and eating pathology was mediated by normative beliefs about the propriety of emotional expressions. In other words, a negative attitude towards emotional expression, which may be procured from an invalidating environment, presented a risk factor for disordered eating.
One implication of these findings is that childhood environments contribute to the way in which we understand and respond to our internal states, such as emotions or, by extension, other internal biochemical signals such as hunger.
Conditioning Appetite Cues
All animals, including human beings, require food to maintain homeostasis. As such, the nature of food acquisition is the product of a learned response between physiological cues signalling the requirement of food intake, and environmental stimuli signalling the presence of food. However, not all appetite cues are internally produced, nor do they exert the same influence on eating behaviour.
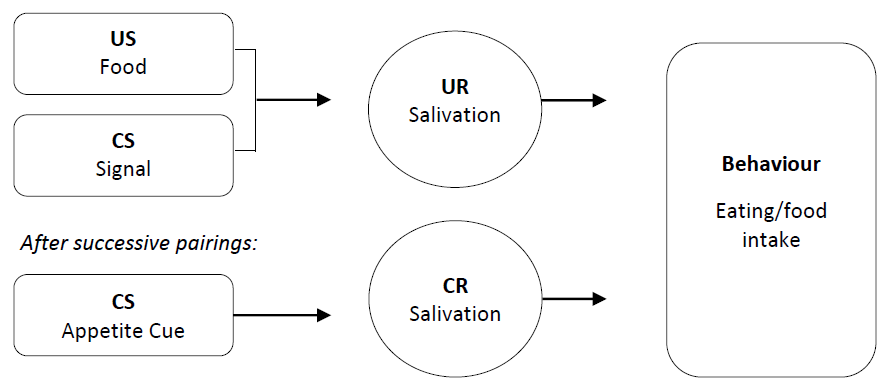
Specifically, cues may elicit appetitive processes independent from any physical sensations of hunger. This was illustrated as part of the pioneering work of Ivan Pavlov, who found that biochemical appetitive processes, such as salivation and gastric secretions, were elicited by a stimulus which had been paired with food but subsequently presented without it (Todes, 2014). As shown in Figure 1, food is an unconditioned stimulus (US) that unconditionally elicits a physiological reaction (UR), yet upon frequent pairings of food with some signal, that signal becomes an appetite cue (CS) which elicits the same physiological reaction (Jansen, 1998).
For purposes of homeostasis, the appetite cue that elicits the CR is an internal physiological sensation signalling either hunger or satiety (Schachter, 1968). Thus, disordered eating can be understood as a failure to regulate food intake in response to internal cues.
Specifically, cues may elicit appetitive processes independent from any physical sensations of hunger. This was illustrated as part of the pioneering work of Ivan Pavlov, who found that biochemical appetitive processes, such as salivation and gastric secretions, were elicited by a stimulus which had been paired with food but subsequently presented without it (Todes, 2014). As shown in Figure 1, food is an unconditioned stimulus (US) that unconditionally elicits a physiological reaction (UR), yet upon frequent pairings of food with some signal, that signal becomes an appetite cue (CS) which elicits the same physiological reaction (Jansen, 1998).
For purposes of homeostasis, the appetite cue that elicits the CR is an internal physiological sensation signalling either hunger or satiety (Schachter, 1968). Thus, disordered eating can be understood as a failure to regulate food intake in response to internal cues.
External appetite cues
External cues are conditioned from environmental stimuli, and can be understood as either a normative cue signalling social expectations of food intake, or sensory cues which signal the sensory or hedonic appeal of food such as high palatability (Herman & Polivy, 2008).
External cues are associated with increased food intake and reduced self-monitoring of consumption amounts (Wansink, 2010). This may be because the influence of normative cues often occurs outside of conscious awareness. For instance, a meta-analysis by Lenny R. Vartanian, Spanos, Herman, and Polivy (2015) found a moderate positive correlation (r = .39) between the amount of food consumed by participants across 38 studies, and that consumed by study confederates. However, the authors suggest that social models exert a greater effect on intake restriction rather than increased consumption. Further, it has been suggested that a tendency to misattribute the influence of external cues on consumption to personal factors such as self-control may be due to self-control being regarded as a social virtue (L. R. Vartanian et al., 2017). Regardless, it is apparent that social modelling is more likely to inhibit intake rather than increase it.
External cues are associated with increased food intake and reduced self-monitoring of consumption amounts (Wansink, 2010). This may be because the influence of normative cues often occurs outside of conscious awareness. For instance, a meta-analysis by Lenny R. Vartanian, Spanos, Herman, and Polivy (2015) found a moderate positive correlation (r = .39) between the amount of food consumed by participants across 38 studies, and that consumed by study confederates. However, the authors suggest that social models exert a greater effect on intake restriction rather than increased consumption. Further, it has been suggested that a tendency to misattribute the influence of external cues on consumption to personal factors such as self-control may be due to self-control being regarded as a social virtue (L. R. Vartanian et al., 2017). Regardless, it is apparent that social modelling is more likely to inhibit intake rather than increase it.
By contrast, it is evident that environmental signals conditioned into appetite cues increase food consumption. For instance, larger serving- and portion-sizes have been associated with increased consumption (see Wansink, 2010 for a discussion). A meta-analysis by Zlatevska, Dubelaar, and Holden (2014) found that a doubled portion size was associated with an average increase in consumption by 35%, but the relationship was curvilinear as the effect diminished when portion size reached a certain threshold. In addition, Reppucci and Petrovich (2012) found that an audible tone conditioned into an appetite cue for one group of rats resulted in increased intake upon cue exposure compared to exposure among the non-conditioned group.
Lastly, some environmental signals may distract an individual’s awareness from internal sensations produced by eating food, and this results in increased food intake. For example, a study comparing intake in scenarios which included television watching, sitting in a driving simulator, or conversing with a researcher found that participants in the television condition ate more crisps than the other two conditions (Ogden et al., 2013).
Lastly, some environmental signals may distract an individual’s awareness from internal sensations produced by eating food, and this results in increased food intake. For example, a study comparing intake in scenarios which included television watching, sitting in a driving simulator, or conversing with a researcher found that participants in the television condition ate more crisps than the other two conditions (Ogden et al., 2013).
Sensory perception has also been shown to act as an external appetite cue. McCrickerd and Forde (2016) provide a detailed overview on how sensory cues, such as high palatability, influence consumption. They outline that sensory cues; in the form of visual, olfactory, taste, and texture cues, signal both the food as a US and prior sensory experiences associated with eating that food. In this way, the smell of a food known to be extremely pleasant to an individual elicits a conditioned response associated with its consumption – producing a desire or craving for that pleasant sensation. Sensory cues may also override internal signals of satiety, resulting in increased intake.
A conceptual review by Bilman, van Kleef, and van Trijp (2017) argued that consumption of highly palatable food results in reward centres of the brain being activated rather than the hypothalamus, which is implicated in facilitating satiety signals. This indicates that food eaten in response to high palatability is motivated by reward-seeking intentions, rather than genuine physical need for caloric intake. This was found in a virtual reality study where some virtual rooms were paired with real chocolate, participants with elevated eating disorder risk scores were more likely to re-enter the room that had been paired with chocolate when they were given freedom to explore the virtual environment (Astur et al., 2015).
Appetite Cues and Binge Eating
A conceptual review by Bilman, van Kleef, and van Trijp (2017) argued that consumption of highly palatable food results in reward centres of the brain being activated rather than the hypothalamus, which is implicated in facilitating satiety signals. This indicates that food eaten in response to high palatability is motivated by reward-seeking intentions, rather than genuine physical need for caloric intake. This was found in a virtual reality study where some virtual rooms were paired with real chocolate, participants with elevated eating disorder risk scores were more likely to re-enter the room that had been paired with chocolate when they were given freedom to explore the virtual environment (Astur et al., 2015).
Appetite Cues and Binge Eating
Given that food intake is performed in response to appetite cues, it is to be expected that individuals with binge eating related disorders exhibit increased responsiveness to external cues, specifically sensory cues signalling high palatability and thus reward. In addition, it might also be expected that if these individuals consistently fail to respond to internal cues, the signal behind these cues may go unrecognised. In other words, binge eating may be associated with deficits in interoception.
Indeed, both reward-sensitivity and internal signal resistance have been used to explain more general patterns of compulsive over-consumption of highly palatable food (Erlanson-Albertsson, 2005). As a result, binge eating may be understood as an extreme manifestation of this behaviour, explained by the same mechanisms involved in over-eating generally.
Indeed, both reward-sensitivity and internal signal resistance have been used to explain more general patterns of compulsive over-consumption of highly palatable food (Erlanson-Albertsson, 2005). As a result, binge eating may be understood as an extreme manifestation of this behaviour, explained by the same mechanisms involved in over-eating generally.
Interoception and alexithymia
While many definitions of interoception exist within the literature, attendees of a research summit recently agreed to define it as “…the process by which the nervous system senses, interprets, and integrates signals originating from within the body, providing a moment-by-moment mapping of the body’s internal landscape across conscious and unconscious levels” (Khalsa et al., 2018, p. 501). This outlines the integral role of interoception in regulatory functions necessary to maintain homeostasis. Indeed, interoceptive deficits have been associated with a range of mental disorders throughout the lifespan, and has also been suggested as the oft-posited ‘p-factor’ underlying susceptibility to all forms of psychopathology (Murphy, Brewer, Catmur, & Bird, 2017). For the purposes of food intake, it is evident that accurate interoceptive abilities are necessary to ensure adaptive eating behaviour.
In line with the classical conditioning model illustrated above, the conditioning of a physiological signal into an appetite cue requires awareness and recognition of the internal sensations that the signal produces. Interoceptive abilities consist of three distinct factors, as detailed by Garfinkel, Seth, Barrett, Suzuki, and Critchley (2015). Interoceptive accuracy/sensitivity refers to the accurate detection of internal states. Interoceptive sensibility is the degree to which individuals focus on their internal states as a matter of habit. Lastly, interoceptive awareness is a metacognitive function referring to the awareness of one’s own level of interoceptive accuracy.
In line with the classical conditioning model illustrated above, the conditioning of a physiological signal into an appetite cue requires awareness and recognition of the internal sensations that the signal produces. Interoceptive abilities consist of three distinct factors, as detailed by Garfinkel, Seth, Barrett, Suzuki, and Critchley (2015). Interoceptive accuracy/sensitivity refers to the accurate detection of internal states. Interoceptive sensibility is the degree to which individuals focus on their internal states as a matter of habit. Lastly, interoceptive awareness is a metacognitive function referring to the awareness of one’s own level of interoceptive accuracy.
In addition, it is likely that individuals with high levels of interoceptive awareness would also exhibit high interoceptive sensibility, given that consistent reflection of internal states would make those signals more salient. For this reason, heightened interoception has been associated with anxiety and panic disorders (Murphy et al., 2017). This illustrates that interoception may accommodate excessive attention towards internal physiological processes, such as anxiety symptoms, which amplifies their perceived intensity. In addition, Young et al. (2017) found that, among individuals who engaged in eating for emotional rather than physical reasons, physiological signals were produced but those individuals displayed inhibited interoceptive awareness. This illustrates the necessity of conditioning in understanding appetite, as it is not apparent that physiological signals regulate appetite by default.
Unfortunately, interoception remains under-studied in relation to binge eating. Alexithymia, by contrast, is more frequently studied in these contexts than interoception. Alexithymia refers to a difficulty in recognising and describing one’s own internal states, and has been conceptualised by its absence of interoceptive awareness (Brewer, Cook, & Bird, 2016; Murphy et al., 2017). While the two constructs do not represent opposite poles of the same construct, a meta-analysis of the effect of interoceptive deficits in eating disorders found that alexithymia was a significant contributor to its effect size (Jenkinson, Taylor, & Laws, 2018).
Unfortunately, interoception remains under-studied in relation to binge eating. Alexithymia, by contrast, is more frequently studied in these contexts than interoception. Alexithymia refers to a difficulty in recognising and describing one’s own internal states, and has been conceptualised by its absence of interoceptive awareness (Brewer, Cook, & Bird, 2016; Murphy et al., 2017). While the two constructs do not represent opposite poles of the same construct, a meta-analysis of the effect of interoceptive deficits in eating disorders found that alexithymia was a significant contributor to its effect size (Jenkinson, Taylor, & Laws, 2018).
Regarding eating disorders, alexithymia has been associated with excessive food intake. For instance, a French study on women with BED found that alexithymia was a larger predictor of emotional eating compared to a control group (Pinaquy, Chabrol, Simon, Louvet, & Barbe, 2003). This is consistent with the conditioning model in two ways. Firstly, the presence of emotional eating indicates that food is being consumed as a reward, in response to external sensory cues signalling high palatability. Secondly, the presence of alexithymia suggests an inability to recognise and respond to internal signals which require interoceptive awareness to detect. This latter point is further supported by findings that individuals with BED consume greater amounts of food before reporting similar amounts of satiety as control groups (Sysko, Devlin, Walsh, Zimmerli, & Kissileff, 2007).
In this way, we may understand that the internal cue signalling satiety must be more salient among those with BED before it is recognised. This is also in line with findings that interoception makes internal sensations more salient, whereas an absence of interoceptive awareness makes renders those signals harder to detect.
In this way, we may understand that the internal cue signalling satiety must be more salient among those with BED before it is recognised. This is also in line with findings that interoception makes internal sensations more salient, whereas an absence of interoceptive awareness makes renders those signals harder to detect.
How might external cues be conditioned among those with binge eating behaviours? The aetiological model for BPD by Linehan (1993) suggests that children who are not able to safely express their emotions in the home environment do not learn how to label, and thus regulate, these responses as they arise. From this, it may be inferred that invalidation fosters alexithymia via interoceptive inhibition. In other words, a child being raised in such environments may not acquire much familiarity with their internal landscape, such as affective states or hunger signals. However, there is no known work in the literature to date which has directly investigated the role of invalidation in contributing towards alexithymia or inhibiting the normal development of interoceptive abilities.
Therefore, it can only be theorised from the classical conditioning model of binge eating coupled with the literature on invalidation, that invalidating environments act against the conditioning of internal appetite cues. In addition, given findings of food-as-reward among binge eaters, this can be understood as a form of external emotional regulation – hence the relationship with emotional eating and interoceptive deficits. However, it must be emphasised that these explanatory accounts are only theoretical and require empirical support.
Therefore, it can only be theorised from the classical conditioning model of binge eating coupled with the literature on invalidation, that invalidating environments act against the conditioning of internal appetite cues. In addition, given findings of food-as-reward among binge eaters, this can be understood as a form of external emotional regulation – hence the relationship with emotional eating and interoceptive deficits. However, it must be emphasised that these explanatory accounts are only theoretical and require empirical support.
Binge eating and external cue reactivity
Further, Jansen’s model also posits that binge eating is associated with increased physiological and biochemical reactivity to external sensory cues (Jansen, 1998). In other words, binge eaters are expected to exhibit greater food cravings upon exposure to sensory cues, and the responsiveness towards these cues precedes eating behaviour, as shown in Figure 2. There has since been some support for this prediction, both direct and indirect.
A study on swallowing reactions upon presentation of hedonic food cues by Meyer, Risbrough, Liang, and Boutelle (2015) found that overweight participants swallowed more in response to a cue paired with chocolate than a water cue, compared to lean participants. Although this study did not measure average food intake by participants as researchers opted to measure Body Mass Index (BMI) instead, they inferred that the higher BMI participants ate more in response to external cues than those who were leaner.
This is consistent with the conditioning model by illustrating increased physiological responsiveness to external cues in individuals who may consume greater amounts of food than others.
A study on swallowing reactions upon presentation of hedonic food cues by Meyer, Risbrough, Liang, and Boutelle (2015) found that overweight participants swallowed more in response to a cue paired with chocolate than a water cue, compared to lean participants. Although this study did not measure average food intake by participants as researchers opted to measure Body Mass Index (BMI) instead, they inferred that the higher BMI participants ate more in response to external cues than those who were leaner.
This is consistent with the conditioning model by illustrating increased physiological responsiveness to external cues in individuals who may consume greater amounts of food than others.

Direct support for increased external cue reactivity comes from a study on a group of individuals with BN and BED which found that, upon exposure to a video clip presenting palatable food items, this group reported greater pre- and post-exposure ratings of food cravings, as well as a steeper increase in craving measures post-exposure than a control group (Meule et al., 2018). In addition, studies have found that exposure to external cues by those with BN is associated with activation of neural regions implicated in reward sensitivity. For example, an fMRI study which presented photos of food items to individuals with BN, Anorexia Nervosa (AN), and healthy controls (HC), found that BN participants exhibited greater activity in reward regions of the brain as well as increased activation in regions associated with motor responsivity (Brooks et al., 2011). The authors suggested that motor activation indicated increased appetitive response to food cues, however the sample size of BN participants (n = 8) limited the power of the study. More research is needed in this area to bolster support for the notion that binge eaters exhibit greater reactivity to external cues than other individuals.
Such findings may also help inform common assumptions that over-eating is a failure of top-down self-control, given the different degrees of responsivity to external cues. In other words, it may be inaccurate to characterise excessive food intake as a failure to deploy self-control if the physiological reaction to be controlled is substantially greater among those who binge eat. Despite this, it is apparent the efficacy of interventions may hinge on facilitating the conditioning of, and behavioural response to, internal appetite cues.
Interoceptive Conditioning
The object of conscious attention has been shown to influence the effect of conditioning processes in studies of interoceptive faculties. For instance, Raes and De Raedt (2011) found that participants who were primed with interoceptive awareness, by listening to their own heartbeat, displayed increased response times in a conditioned spatial cueing task. This illustrates that the valence associated with a stimulus, whether desirable or aversive, is enhanced by increased attention towards it. In terms of interoceptive awareness, this suggests that exercises which increase attention towards internal states makes those signals more salient, which further facilitates responsiveness. Interoceptive awareness may be fostered early in life, as Quattrocki and Friston (2014) suggest that early attachment between infant and caregiver may be strengthened by an association between caregiver eye-contact and feelings of warmth. Thus, this association requires interoception to register the internal sensation of warmth. Regarding invalidating childhood environments, it may be speculated that opportunities to foster these associations are rarely experienced. Given this, we may understand interventions which facilitate responsiveness to internal cues is a form of conditioning which involves interoception.
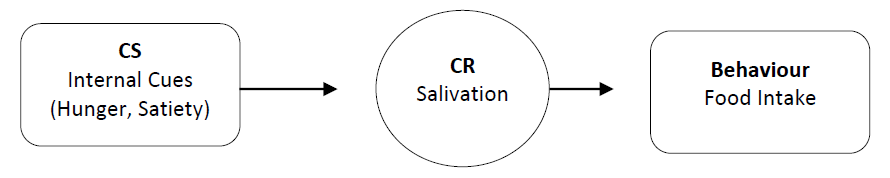
In a review of interoception and conditioning, Van Diest (2019) concludes that interoceptive conditioning is a special case of classical conditioning. Specifically, interoceptive conditioning involves learned associations with interoceptive stimuli including feelings of thirst or hunger. Figure 3 illustrates the conditioning process of internal cues via interoceptive conditioning. In addition, the author summarises two findings within the literature on the topic which are relevant to understanding conditioning of internal cues: interoceptive conditioning typically occurs unconsciously and is more resistant to extinction that exteroceptive conditioning.
Firstly, the finding that interoceptive conditioning is typically an unconscious process fits with models indicating that it begins in infancy. Secondly, it suggests that binge eating interventions which facilitate interoceptive conditioning may be more successful in the long term. This may be because interoceptive conditioning is not a stimulus-dependent as exteroceptive conditioning. Where signals of high palatability are a conditioned response to a specific food, intake regulation by internal cues are not restricted to any type of food.
Firstly, the finding that interoceptive conditioning is typically an unconscious process fits with models indicating that it begins in infancy. Secondly, it suggests that binge eating interventions which facilitate interoceptive conditioning may be more successful in the long term. This may be because interoceptive conditioning is not a stimulus-dependent as exteroceptive conditioning. Where signals of high palatability are a conditioned response to a specific food, intake regulation by internal cues are not restricted to any type of food.
Interoception and Intuitive Eating
If a failure to recognise internal signals is a defining characteristic of binge eating behaviour, how is it possible to facilitate interoceptive conditioning? If physiological signals of hunger and satiety are to be conditioned into appetite cues, it is evident that these signals must be detectable. However, as food intake, performed for purposes of homeostasis, is a behavioural response to a physiological signal of hunger then it is likely that fasting makes this signal more salient. This was found in a study by Herbert et al. (2012) on short term food deprivation on interoceptive awareness as measured by a heartbeat tracking task. Specifically, the authors found that fasting brought about changes to cardiac activity that, upon encouraging participants to focus upon their heartbeat, also resulted in increases in self-reported measures of hunger feelings. In this way, increased interoceptive awareness resulted in amplified hunger signals. In addition, interoceptive sensitivity is associated with Intuitive Eating (IE) habits, eating behaviour performed in response to internal cues, as shown by Herbert, Blechert, Hautzinger, Matthias, and Herbert (2013). The authors found that participants with higher scores on the Intuitive Eating Scale (IES) were more likely to have a lower BMI and increased interoceptive sensitivity, the latter being measured by heartbeat detection.
Intuitive Eating is not always defined by its absence, and several studies have sought to investigate the nature of IE among the general population. A factor analytic study found that all eating behaviours consisted of four components with the largest component, ‘attuned eating’, consisting primarily of intuitive and mindful eating practices (Kerin, Webb, & Zimmer-Gembeck, 2019). A study using data from population-based survey in Minnesota found that responses relating to IE practices (“I stop eating when I am full”) were inversely associated with BMI among both men and women (Denny, Loth, Eisenberg, & Neumark-Sztainer, 2013). Further, a correlational study on IE among Australian adolescent girls found that IE scores were moderately correlated with measures of both self- and social-acceptance of body appearance, with the largest correlation between IE and body appreciation (r = .53, p < .001).
This is illustrative of the role of the social environment in fostering healthy eating habits, albeit mediated by body acceptance. In addition, data from a study on Swiss adults found significant correlations between IE scores and excessive food intake, BMI, physical activity level (Horwath, Hagmann, & Hartmann, 2019). However, the authors did not find a significant relationship between IE measures and the quality of diet. This is unsurprising as IE refers to food intake performed in response to internal cues and does not include the quality of the food itself.
This is illustrative of the role of the social environment in fostering healthy eating habits, albeit mediated by body acceptance. In addition, data from a study on Swiss adults found significant correlations between IE scores and excessive food intake, BMI, physical activity level (Horwath, Hagmann, & Hartmann, 2019). However, the authors did not find a significant relationship between IE measures and the quality of diet. This is unsurprising as IE refers to food intake performed in response to internal cues and does not include the quality of the food itself.
IE is a central component of behavioural interventions for binge eating behaviour. For example, the core focus of CBT-A is on the role of appetitive conditioning in binge episodes, and a treatment goal is the facilitation of interoceptive awareness (Virginia V. W. McIntosh et al., 2007). Specifically, appetite focused versions of CBT replaces typical CBT tasks such as maintaining food diaries, with attention towards internal states (Dicker & Craighead, 2004). The developers of CBT-A conceptualise internal appetite cues with the analogy of a volume dial, where certain behaviours and foods result in the volume being turned down, and the goal of the intervention is to turn the dial up. While CBT-A does not facilitate interoceptive conditioning by short term fasting, it does encourage the individual to monitor their appetite, particularly to noticing changes in appetite following food intake. This is fostered by strict monitoring of food intake, to compare changes in internal signals in relation to quantities consumed. Monitoring of thoughts, feelings, and cues is also encouraged to prevent reverting to automatic responses to external cues, and this may also foster the development of interoceptive awareness – however more work is required to measure CBT-A on changes in interoceptive abilities.
CBT-A incorporates another important finding in the literature: different foods have varying degrees of influence on the ‘volume’ of internal signals of satiety. A review by Stevenson, Mahmut, and Rooney (2015) found indirect support for the effect of diet on interoceptive awareness among rats. They found that rats who were given a diet higher in fat and sugar (HFS) to other rats displayed impairments on cognitive tasks requiring executive control, as well as failing to distinguish between external and internal appetite cues. The authors note that while similar studies on humans are difficult to conduct, those that have used the HFS diet report that individuals on these diets consume more calories before indicating fullness.
For this reason, CBT-A encourages food choices that are known to increase feelings of satiety yet are less energy-dense than food typically eaten in a binge session. Specifically, the three principles of food choice to promote satiety are choosing those that are greater in volume, increasing protein intake, and choosing carbohydrates with a lower glycaemic index to ensure greater energy release over time.
For this reason, CBT-A encourages food choices that are known to increase feelings of satiety yet are less energy-dense than food typically eaten in a binge session. Specifically, the three principles of food choice to promote satiety are choosing those that are greater in volume, increasing protein intake, and choosing carbohydrates with a lower glycaemic index to ensure greater energy release over time.
Given the recency of its development, publications on the efficacy of CBT-A are limited. However, a study comparing CBT, CBT-A, and Schema Therapy for binge eating found no significant difference in the number of binge episodes at 12-month follow-up between intervention conditions (V. V. W. McIntosh et al., 2016). However, the authors speculate that treatment length was atypical for some of the interventions used, and the study may have suffered from limited statistical power given the dropout rate. In addition, it is not clear that individuals who undergo CBT-A treatment experience interoceptive conditioning given the absence of any measure of interoceptive awareness as part of the treatment programme. Furthermore, this study measured efficacy as it related to binge episode frequency, rather than a measure of overall caloric intake given that this is not a key focus of binge eating interventions. This limitation was also noted in a qualitative study comparing appetite focused CBT among 4 individuals with BN to waitlist controls (Dicker & Craighead, 2004). Specifically, the authors note that while all 4 individuals successfully recovered at follow-up, they had not measured further changes implied by the underlying rationale around interoception.
Evaluating the efficacy of IE interventions is problematic given limited publications on the subject. Indeed, it has been noted that while many studies have presented impressive correlations between IE and positive outcomes, there is limited experimental support for IE as an intervention (Warren, Smith, & Ashwell, 2017).
Evaluating the efficacy of IE interventions is problematic given limited publications on the subject. Indeed, it has been noted that while many studies have presented impressive correlations between IE and positive outcomes, there is limited experimental support for IE as an intervention (Warren, Smith, & Ashwell, 2017).
Extinction of external cues
While interoceptive conditioning is likely to be a critical component of efficacious binge eating interventions, it would be a mistake to regard IE as a single factor solution. In her original model outlining the conditioning of binge eating behaviours, Jansen (1998) emphasised that conditioning internal cues does not extinguish the conditioned response of external cues. In other words, IE does not replace reactivity to external cues, such as high palatability, and this process is a defining characteristic of binge eating behaviour. This is indirectly supported by findings that individuals with high IE scores were more likely to increase their consumption of pasta if they were given a larger plate, compared to those lower on IE (Anderson, Schaumberg, Anderson, & Reilly, 2015). This suggests that external cue responsivity not only lingers after interoceptive conditioning, but that cue reactivity may be context dependent.
As a result, interventions incorporating IE will also need to address susceptibility to external cue reactivity. While this study found evidence for retention of normative cues, some studies have investigated the efficacy of CBT for BN individuals as a measure of binge cue reactivity. For instance, Carter, McIntosh, Joyce, Frampton, and Bulik (2006) studied cue reactivity in the form of self-reports of cravings among individuals with BN undergoing standard CBT at three time points encompassing treatment. While the authors do not specify the content of each cue, it is likely that they were sensory cues given their role in contributing to binge eating. Results indicated a significant reduction in cue reactivity among post-treatment scores, as well as at a 6-month follow-up. This highlights the potential utility of exposure as a supplement to interoceptive conditioning.
As a result, interventions incorporating IE will also need to address susceptibility to external cue reactivity. While this study found evidence for retention of normative cues, some studies have investigated the efficacy of CBT for BN individuals as a measure of binge cue reactivity. For instance, Carter, McIntosh, Joyce, Frampton, and Bulik (2006) studied cue reactivity in the form of self-reports of cravings among individuals with BN undergoing standard CBT at three time points encompassing treatment. While the authors do not specify the content of each cue, it is likely that they were sensory cues given their role in contributing to binge eating. Results indicated a significant reduction in cue reactivity among post-treatment scores, as well as at a 6-month follow-up. This highlights the potential utility of exposure as a supplement to interoceptive conditioning.
Such findings are unsurprising as it has been suggested that reduced reactivity to cues may result from exposure interventions (Jansen, 1998; van den Akker, Schyns, & Jansen, 2018). In developing her model, Jansen was informed by the literature on in vivo cue exposure on reducing cravings among individuals with substance abuse problems. This was also informed by a prior experiment on cue exposure among six individuals with BN (Jansen, Broekmate, & Heymans, 1992). Researchers presented participants with food items typical of a binge session during exposure trials for an hour, where participants were able to interact with the items without eating them or were free go about some other task in the room but within physical proximity of the stimulus. Results indicated a reduction in binge frequency after six exposure trials, and this reduction held at 12-month follow up.
Thus, exposure interventions coupled with methods of facilitating interoceptive conditioning may maximise the consistency of IE habits. For example, a within-groups study on a sample of non-clinical binge eaters measured the effect of an intervention that included both interoceptive conditioning and external cue exposure, in the form of in vivo exposure to foods known to induce cravings, on measures of food responsiveness and overeating episodes (Boutelle, Knatz, Carlson, Bergmann, & Peterson, 2017). Multivariate analyses found significant decreases in the number of binge episodes post-treatment and at 3-month follow-up, as well as significant decreases in sensory cue responsiveness at both time points. However, with a sample of n = 17, it must be noted that statistical power may limit the generalisability of this within-subjects design. Despite this, similar main effects for cue exposure have been found in a between-subjects design of n = 22 in the exposure condition, and n = 23 in a control group (Schyns, van den Akker, Roefs, Houben, & Jansen, 2019). Results indicated that while participants in the exposure condition exhibited significant reductions in the frequency of snacking on exposed foods, the main effect of exposure was mediated by cognitions around self-control, and exposure did not generalise to non-exposed foods. This may prove to be a financial and practical challenge in the administration of exposure interventions of this kind, as its efficacy may hinge on exposure to each food conditioned into sensory cues.
However, recent advances in virtual reality methods of cue exposure may overcome this barrier. Recent findings suggest that virtual cue exposure may be successful in preventing binge eating episodes among clinical samples. For instance, Spanish studies using virtual cue exposure on individuals with BN and BED found a significant reduction in binge episodes among the exposure group compared to a group receiving additional CBT sessions, and this reduction was consistent at 6-month follow-up (Ferrer-Garcia et al., 2017; Ferrer-Garcia et al., 2019).
Summary and Discussion
In sum, the treatment of eating disorders has become an urgent issue in New Zealand, and it is imperative that interventions target maintaining factors behind binge eating behaviour. Binge eating is the result of food intake in response to external appetite cues signalling the hedonic value of food, as well as decreased responsivity towards internal cues signalling physiological requirement. Interventions which facilitate the interoceptive conditioning of these internal signals into internal appetite cues are necessary to ensure intuitive eating habits, and CBT-A is one such example. In addition, interoceptive conditioning does not correspond to external cue extinction, and exposure interventions designed to facilitate cue habituation is necessary to prevent binge sessions.
There are several limitations in the literature which informed this review. Firstly, there is only been one clinical trial to date on the efficacy of CBT-A compared to other treatments for binge eating, and more work is required to support this intervention given its substantial theoretical support. In addition, measuring the efficacy of IE interventions may need to be re-conceptualised to gauge changes in the conditioning of cues as well the reactions they elicit. While a reduction in binge episodes is a desirable outcome, it does not provide concrete support for the extinction of external cue effects or for strengthened interoceptive abilities.
Studies investigating binge eating interventions may benefit from measuring both factors. Further, interoceptive awareness has been shown to be facilitated by short term fasting, however no interventions incorporate this strategy as part of the interoceptive conditioning process. Future work may compare the strengthening of interoceptive awareness between induction by fasting, and induction by self-monitoring processes such as conscious awareness or mindfulness-based activities.
Studies investigating binge eating interventions may benefit from measuring both factors. Further, interoceptive awareness has been shown to be facilitated by short term fasting, however no interventions incorporate this strategy as part of the interoceptive conditioning process. Future work may compare the strengthening of interoceptive awareness between induction by fasting, and induction by self-monitoring processes such as conscious awareness or mindfulness-based activities.
Secondly, childhood invalidation has been associated with the onset of eating disorders, such as those involving binge eating, yet descriptions outlining how these environments contribute towards binge eating behaviour are absent in the literature. While it is possible that invalidation of the expression of internal states may result in a failure to identify internal states over time, it is also possible that these environments invalidate hunger signals more directly and that this process hinders the conditioning of internal cues.
Regardless, more work is required to investigate the role of invalidation on eating psychopathology from within the classical conditioning paradigm. Third, many of the studies in the literature have gauged changes in BMI or weight as evidence of intervention success. While weight gain may correspond to over-eating more generally, it is not a reliable gauge of current eating habits, and studies may provide more precise measurements of an interventions’ efficacy by measuring changes in average caloric intake.
Regardless, more work is required to investigate the role of invalidation on eating psychopathology from within the classical conditioning paradigm. Third, many of the studies in the literature have gauged changes in BMI or weight as evidence of intervention success. While weight gain may correspond to over-eating more generally, it is not a reliable gauge of current eating habits, and studies may provide more precise measurements of an interventions’ efficacy by measuring changes in average caloric intake.
Lastly, this review has outlined the necessity of cue exposure in reducing external cue reactivity. Cue reactivity among binge eaters is a topic which has received little attention, and more work is required to understand the nature of physiological reactions among these individuals compared with intuitive eaters. In addition, neurological studies may illuminate changes in brain processes associated with exposure to food. For instance, sensory cues have been shown to activate reward regions in the brain, and it is uncertain whether extinction trials correspond to a reduction of activity in these areas. While cue exposure has emerged as a viable candidate in reducing reactivity associated with sensory cues, it remains a possibility that IE alters the way food is perceived. In other words, subsequent eating habits performed out of physical requirements rather than emotional may correspond to food stimuli being conditioned as food-as-nourishment rather than food-as-reward.
Further, as in vivo exposure may prove difficult in tailoring interventions to individual needs, virtual reality technology has recently provided support for virtual cue exposure. In the current digital age, many individuals possess electronic devices on their person which may assist in making cue exposure widely accessible. Future research may benefit from investigating the feasibility of IE interventions which include interoceptive conditioning tasks, as well as exposure to external cues. As access to interventions has been mentioned as a barrier to many with eating disorders in New Zealand, such an approach may prove beneficial to those who are not able or willing to initiate contact with intervention services.
References
Further, as in vivo exposure may prove difficult in tailoring interventions to individual needs, virtual reality technology has recently provided support for virtual cue exposure. In the current digital age, many individuals possess electronic devices on their person which may assist in making cue exposure widely accessible. Future research may benefit from investigating the feasibility of IE interventions which include interoceptive conditioning tasks, as well as exposure to external cues. As access to interventions has been mentioned as a barrier to many with eating disorders in New Zealand, such an approach may prove beneficial to those who are not able or willing to initiate contact with intervention services.
References
Afifi, T. O., Sareen, J., Fortier, J., Taillieu, T., Turner, S., Cheung, K., & Henriksen, C. A. (2017). Child maltreatment and eating disorders among men and women in adulthood: Results from a nationally representative United States sample. International Journal of Eating Disorders, 50(11), 1281-1296. doi:10.1002/eat.22783
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders DSM-5 (Fifth Edition ed.). Washington, DC: American Psychiatric Publishing.
Anderson, D. A., Schaumberg, K., Anderson, L. M., & Reilly, E. E. (2015). Is level of intuitive eating associated with plate size effects? Eating Behaviors, 18, 125-130. doi:10.1016/j.eatbeh.2015.05.005
Astur, R. S., Palmisano, A. N., Hudd, E. C., Carew, A. W., Deaton, B. E., Kuhney, F. S., . . . Santos, M. (2015). Pavlovian conditioning to food reward as a function of eating disorder risk. Behavioural Brain Research, 291, 277-282. doi:10.1016/j.bbr.2015.05.016
Bilman, E., van Kleef, E., & van Trijp, H. (2017). External cues challenging the internal appetite control system-Overview and practical implications. Critical Reviews in Food Science and Nutrition, 57(13), 2825-2834. doi:10.1080/10408398.2015.1073140
Boutelle, K. N., Knatz, S., Carlson, J., Bergmann, K., & Peterson, C. B. (2017). An Open Trial Targeting Food Cue Reactivity and Satiety Sensitivity in Overweight and Obese Binge Eaters. Cognitive and Behavioral Practice, 24(3), 363-373. doi:10.1016/j.cbpra.2016.08.003
Brewer, R., Cook, R., & Bird, G. (2016). Alexithymia: a general deficit of interoception. Royal Society of Open Science, 3(10), 150664. doi:10.1098/rsos.150664
Brooks, S. J., O'Daly, O. G., Uher, R., Friederich, H. C., Giampietro, V., Brammer, M., . . . Campbell, I. C. (2011). Differential neural responses to food images in women with bulimia versus anorexia nervosa. PLoS One, 6(7), e22259. doi:10.1371/journal.pone.0022259
Carter, F. A., McIntosh, V. V., Joyce, P. R., Frampton, C. M., & Bulik, C. M. (2006). Cue reactivity in bulimia nervosa: A useful self-report approach. International Journal of Eating Disorders, 39(8), 694-699. doi:10.1002/eat.20331
Denny, K. N., Loth, K., Eisenberg, M. E., & Neumark-Sztainer, D. (2013). Intuitive eating in young adults. Who is doing it, and how is it related to disordered eating behaviors? Appetite, 60(1), 13-19. doi:10.1016/j.appet.2012.09.029
Dicker, S. L., & Craighead, L. W. (2004). Appetite-focused cognitive-behavioral therapy in the treatment of binge eating with purging. Cognitive and Behavioral Practice, 11(2), 213-221. doi:10.1016/S1077-7229(04)80032-4
Erlanson-Albertsson, C. (2005). How palatable food disrupts appetite regulation. Basic & Clinical Pharmacology & Toxicology, 97(2), 61-73. doi:10.1111/j.1742-7843.2005.pto_179.x
Ferrer-Garcia, M., Gutierrez-Maldonado, J., Pla-Sanjuanelo, J., Vilalta-Abella, F., Riva, G., Clerici, M., . . . Dakanalis, A. (2017). A Randomised Controlled Comparison of Second-Level Treatment Approaches for Treatment-Resistant Adults with Bulimia Nervosa and Binge Eating Disorder: Assessing the Benefits of Virtual Reality Cue Exposure Therapy. European Eating Disorders Review, 25(6), 479-490. doi:10.1002/erv.2538
Ferrer-Garcia, M., Pla-Sanjuanelo, J., Dakanalis, A., Vilalta-Abella, F., Riva, G., Fernandez-Aranda, F., . . . Gutierrez-Maldonado, J. (2019). A Randomized Trial of Virtual Reality-Based Cue Exposure Second-Level Therapy and Cognitive Behavior Second-Level Therapy for Bulimia Nervosa and Binge-Eating Disorder: Outcome at Six-Month Followup. Cyberpsychology, behavior, and social networking, 22(1), 60-68. doi:10.1089/cyber.2017.0675
Garfinkel, S. N., Seth, A. K., Barrett, A. B., Suzuki, K., & Critchley, H. D. (2015). Knowing your own heart: distinguishing interoceptive accuracy from interoceptive awareness. Biological Psychology, 104, 65-74. doi:10.1016/j.biopsycho.2014.11.004
Haslam, M., Arcelus, J., Farrow, C., & Meyer, C. (2012). Attitudes towards emotional expression mediate the relationship between childhood invalidation and adult eating concern. European Eating Disorders Review, 20(6), 510-514. doi:10.1002/erv.2198
Herbert, B. M., Blechert, J., Hautzinger, M., Matthias, E., & Herbert, C. (2013). Intuitive eating is associated with interoceptive sensitivity. Effects on body mass index. Appetite, 70, 22-30. doi:10.1016/j.appet.2013.06.082
Herbert, B. M., Herbert, C., Pollatos, O., Weimer, K., Enck, P., Sauer, H., & Zipfel, S. (2012). Effects of short-term food deprivation on interoceptive awareness, feelings and autonomic cardiac activity. Biological Psychology, 89(1), 71-79. doi:10.1016/j.biopsycho.2011.09.004
Herman, C. P., & Polivy, J. (2008). External cues in the control of food intake in humans: the sensory-normative distinction. Physiology & Behavior, 94(5), 722-728. doi:10.1016/j.physbeh.2008.04.014
Horwath, C., Hagmann, D., & Hartmann, C. (2019). Intuitive eating and food intake in men and women: Results from the Swiss food panel study. Appetite, 135, 61-71. doi:10.1016/j.appet.2018.12.036
Jansen, A. (1998). A learning model of binge eating: Cue reactivity and cue exposure. Behaviour Research and Therapy, 36(3), 257-272. doi:10.1016/s0005-7967(98)00055-2
Jansen, A., Broekmate, J., & Heymans, M. (1992). Cue-exposure vs self-control in the treatment of binge eating: A pilot study. Behaviour Research and Therapy, 30(3), 235-241. doi:10.1016/0005-7967(92)90069-s
Jenkinson, P. M., Taylor, L., & Laws, K. R. (2018). Self-reported interoceptive deficits in eating disorders: A meta-analysis of studies using the eating disorder inventory. Journal of Psychosomatic Research, 110, 38-45. doi:10.1016/j.jpsychores.2018.04.005
Kerin, J. L., Webb, H. J., & Zimmer-Gembeck, M. J. (2019). Intuitive, mindful, emotional, external and regulatory eating behaviours and beliefs: An investigation of the core components. Appetite, 132, 139-146. doi:10.1016/j.appet.2018.10.011
Khalsa, S. S., Adolphs, R., Cameron, O. G., Critchley, H. D., Davenport, P. W., Feinstein, J. S., . . . Interoception Summit, p. (2018). Interoception and Mental Health: A Roadmap. Biological Psychiatry Cognitive Neuroscience Neuroimaging, 3(6), 501-513. doi:10.1016/j.bpsc.2017.12.004
Linardon, J., Fairburn, C. G., Fitzsimmons-Craft, E. E., Wilfley, D. E., & Brennan, L. (2017). The empirical status of the third-wave behaviour therapies for the treatment of eating disorders: A systematic review. Clinical Psychology Review, 58, 125-140. doi:10.1016/j.cpr.2017.10.005
Linardon, J., Wade, T. D., de la Piedad Garcia, X., & Brennan, L. (2017). The efficacy of cognitive-behavioral therapy for eating disorders: A systematic review and meta-analysis. Journal of Consulting and Clinical Psychology, 85(11), 1080-1094. doi:10.1037/ccp0000245
Linehan, M. (1993). Cognitive-Behavioural Treatment of Borderline Personality Disorder. New York: Guildford Press.
McCrickerd, K., & Forde, C. G. (2016). Sensory influences on food intake control: moving beyond palatability. Obesity Reviews, 17(1), 18-29. doi:10.1111/obr.12340
McIntosh, V. V. W., Jordan, J., Carter, J. D., Frampton, C. M. A., McKenzie, J. M., Latner, J. D., & Joyce, P. R. (2016). Psychotherapy for transdiagnostic binge eating: A randomized controlled trial of cognitive-behavioural therapy, appetite-focused cognitive-behavioural therapy, and schema therapy. Psychiatry Research, 240, 412-420. doi:10.1016/j.psychres.2016.04.080
McIntosh, V. V. W., Jordan, J., Carter, J. D., Latner, J. D., & Wallace, A. (2007). Appetite focused CBT for binge eating. In J. D. Latner & G. T. Wilson (Eds.), Self-help approaches for obesity and eating disorders: Research and practice. (pp. 325-346). New York, NY, US: Guilford Press.
Mental Health and Addiction Inquiry. (2018). He Ara Oranga: Report of the Government Inquiry into Mental Health and Addiction. Retrieved from Wellington, New Zealand:
Meule, A., Kuppers, C., Harms, L., Friederich, H. C., Schmidt, U., Blechert, J., & Brockmeyer, T. (2018). Food cue-induced craving in individuals with bulimia nervosa and binge-eating disorder. PLoS One, 13(9), e0204151. doi:10.1371/journal.pone.0204151
Meyer, M. D., Risbrough, V. B., Liang, J., & Boutelle, K. N. (2015). Pavlovian conditioning to hedonic food cues in overweight and lean individuals. Appetite, 87, 56-61. doi:10.1016/j.appet.2014.12.002
Ministry of Health. (2008). Future Directions for Eating Disorders Services in New Zealand. Retrieved from Wellington, New Zealand:
Mountford, V., Corstorphine, E., Tomlinson, S., & Waller, G. (2007). Development of a measure to assess invalidating childhood environments in the eating disorders. Eating Behaviors, 8(1), 48-58. doi:10.1016/j.eatbeh.2006.01.003
Murphy, J., Brewer, R., Catmur, C., & Bird, G. (2017). Interoception and psychopathology: A developmental neuroscience perspective. Developmental Cognitive Neuroscience, 23, 45-56. doi:10.1016/j.dcn.2016.12.006
Ogden, J., Coop, N., Cousins, C., Crump, R., Field, L., Hughes, S., & Woodger, N. (2013). Distraction, the desire to eat and food intake. Towards an expanded model of mindless eating. Appetite, 62, 119-126. doi:10.1016/j.appet.2012.11.023
Pinaquy, S., Chabrol, H., Simon, C., Louvet, J. P., & Barbe, P. (2003). Emotional eating, alexithymia, and binge-eating disorder in obese women. Obesity Research, 11(2), 195-201. doi:10.1038/oby.2003.31
Quattrocki, E., & Friston, K. (2014). Autism, oxytocin and interoception. Neuroscience and Biobehavioral Reviews, 47, 410-430. doi:10.1016/j.neubiorev.2014.09.012
Raes, A. K., & De Raedt, R. (2011). Interoceptive awareness and unaware fear conditioning: are subliminal conditioning effects influenced by the manipulation of visceral self-perception? Consciousness and Cognition, 20(4), 1393-1402. doi:10.1016/j.concog.2011.05.009
Reppucci, C. J., & Petrovich, G. D. (2012). Learned food-cue stimulates persistent feeding in sated rats. Appetite, 59(2), 437-447. doi:10.1016/j.appet.2012.06.007
Schachter, S. (1968). Obesity and eating. Internal and external cues differentially affect the eating behavior of obese and normal subjects. Science (New York, N.Y.), 161(3843), 751-756.
Schyns, G., van den Akker, K., Roefs, A., Houben, K., & Jansen, A. (2019). Exposure therapy vs lifestyle intervention to reduce food cue reactivity and binge eating in obesity: A pilot study. Journal of Behavior Therapy and Experimental Psychiatry. doi:10.1016/j.jbtep.2019.01.005
Stevenson, R. J., Mahmut, M., & Rooney, K. (2015). Individual differences in the interoceptive states of hunger, fullness and thirst. Appetite, 95, 44-57. doi:10.1016/j.appet.2015.06.008
Sysko, R., Devlin, M. J., Walsh, B. T., Zimmerli, E., & Kissileff, H. R. (2007). Satiety and test meal intake among women with binge eating disorder. International Journal of Eating Disorders, 40(6), 554-561. doi:10.1002/eat.20384
Tetley, A., Moghaddam, N. G., Dawson, D. L., & Rennoldson, M. (2014). Parental bonding and eating disorders: a systematic review. Eating Behaviors, 15(1), 49-59. doi:10.1016/j.eatbeh.2013.10.008
Todes, D. P. (2014). Ivan Pavlov : A Russian Life in Science. Oxford, [England]: Oxford University Press.
van den Akker, K., Schyns, G., & Jansen, A. (2018). Learned Overeating: Applying Principles of Pavlovian Conditioning to Explain and Treat Overeating. Current Addiction Reports, 5(2), 223-231. doi:10.1007/s40429-018-0207-x
Van Diest, I. (2019). Interoception, conditioning, and fear: The panic threesome. Psychophysiology, 56(8), e13421. doi:10.1111/psyp.13421
Vartanian, L. R., Reily, N. M., Spanos, S., McGuirk, L. C., Herman, C. P., & Polivy, J. (2017). Hunger, taste, and normative cues in predictions about food intake. Appetite, 116, 511-517. doi:10.1016/j.appet.2017.05.044
Vartanian, L. R., Spanos, S., Herman, C. P., & Polivy, J. (2015). Modeling of food intake: a meta-analytic review. Social Influence, 10(3), 119-136. doi:10.1080/15534510.2015.1008037
Wansink, B. (2010). From mindless eating to mindlessly eating better. Physiology & Behavior, 100(5), 454-463. doi:10.1016/j.physbeh.2010.05.003
Warren, J. M., Smith, N., & Ashwell, M. (2017). A structured literature review on the role of mindfulness, mindful eating and intuitive eating in changing eating behaviours: effectiveness and associated potential mechanisms. Nutrition Research Reviews, 30(2), 272-283. doi:10.1017/S0954422417000154
Young, H. A., Williams, C., Pink, A. E., Freegard, G., Owens, A., & Benton, D. (2017). Getting to the heart of the matter: Does aberrant interoceptive processing contribute towards emotional eating? PLoS One, 12(10), e0186312. doi:10.1371/journal.pone.0186312
Zlatevska, N., Dubelaar, C., & Holden, S. S. (2014). Sizing up the Effect of Portion Size on Consumption: A Meta-Analytic Review. Journal of Marketing, 78(3), 140-154. doi:10.1509/jm.12.0303